


Why I Recommend Chlorine Dioxide for Self-Treatment, Especially for Advanced Cancer Patients, and Particularly Those with Late-Stage Breast Cancer(Part II)

Continuing this topic from my last post, my narrative is as follows: 1) Modern medicine can only treat about 10% of human diseases, which is far from sufficient. 2) Chlorine dioxide works through three key mechanisms in the body that allow it to treat up to 50% of human diseases, or even more. 3) Anyone can easily use chlorine dioxide; it isn’t a prescription drug. You don’t need a doctor’s prescription to get it, as it is available as a water treatment or disinfectant agent. Anyone can obtain it at a low cost, and for most cases, purchasing chlorine dioxide to treat 80% of diseases will cost under $100. As I write this post, three late-stage breast cancer patients are under my guidance, using intratumoral chlorine dioxide injections for their large tumors. The therapy is progressing well. Each of these patients had previous experience with chlorine dioxide, having taken MMS/CDS orally for some time. However, due to the large size and spread of their tumors, they needed a more aggressive treatment to quickly ablate their tumors. They are self-treating at home, and from these cases, it’s clear that late-stage breast cancer patients can easily use intratumoral chlorine dioxide injections.
A Deeper Understanding of Cancer Treatment
Cancer refers to a disease where cells in the body lose control over their normal growth and division, continuously multiplying to form tumors. Solid tumors are those that arise from the abnormal proliferation of cells in specific organs, as opposed to hematologic tumors like leukemia. Solid tumors can be benign or malignant, with the latter being cancerous. Malignant solid tumors are invasive, breaching the boundaries of their original tissues, spreading to surrounding areas, and metastasizing to other parts of the body through the blood or lymphatic systems.
Cancer can be caused by various factors, including genetics, environmental exposures (like smoking, chemicals, and radiation), lifestyle choices (such as diet, weight, and exercise), and infections (from certain viruses and bacteria, for instance). The development of cancer can span many years, starting from normal cells to precancerous lesions, and ultimately to malignant tumors.
There are multiple treatment options for cancer, including surgery, radiation therapy, chemotherapy, targeted therapy, and immunotherapy. Surgery is commonly used to remove localized tumors. Radiation and chemotherapy aim to kill or halt the growth of cancer cells. Targeted therapy and immunotherapy are relatively newer treatments that leverage our understanding of the biological characteristics of cancer cells.
However, current treatments have several drawbacks. Surgery can remove tumors but is often ineffective against metastasized cancer. It carries high risks, causes significant trauma to the patient’s body, requires a long recovery period, and may miss tiny cancer cells, leading to recurrence. Radiation and chemotherapy can target cancer cells throughout the body but are imprecise and toxic to normal cells, causing side effects like nausea, vomiting, hair loss, and immunosuppression. Due to the heterogeneity and adaptability of cancer cells, chemotherapy may not eradicate all cancer cells, and drug resistance can develop, reducing the effectiveness over time.
Targeted therapy and immunotherapy represent advancements in cancer treatment, offering more precise targeting of cancer cells or modulating the immune system to recognize and destroy them. However, targeted therapies only work on specific molecular targets, necessitating the expression of these targets on cancer cells. Cancer cells may lose these targets due to genetic mutations, leading to treatment failure. Immunotherapy has shown remarkable results in certain cancers, but not all patients respond, and it can sometimes trigger excessive immune responses that damage healthy tissue.
Both targeted therapy and immunotherapy are important modern cancer treatments, but they both have significant issues with resistance. Targeted therapy inhibits the growth and spread of cancer cells by focusing on unique molecular markers and signaling pathways, while immunotherapy aims to activate or boost the patient’s immune system to identify and eliminate cancer cells.
Resistance to targeted therapy typically develops during treatment, as cancer cells evade the effects of drugs through genetic mutations or changes in expression. For instance, some drugs work by binding to specific proteins on the surface of cancer cells. However, cancer cells may alter the structure of these proteins to reduce drug binding or activate alternative growth signaling pathways to sustain their growth. Additionally, drug pumps within cancer cells can be activated to expel drugs from the cell, reducing the effective drug concentration. Due to these mechanisms, cancer cells can survive under treatment pressure, potentially leading to disease relapse or progression.
Immunotherapy resistance involves the complex interplay between cancer cells and the immune system. Cancer cells can evade immune surveillance through various mechanisms, such as expressing inhibitory molecules like PD-L1 to suppress T cell activity. Immunotherapies, like PD-1 or PD-L1 inhibitors, aim to block these inhibitory signals, but cancer cells may adapt by increasing other immune suppressive pathways. Moreover, other cells in the cancer cell microenvironment, such as regulatory T cells and tumor-associated macrophages, may counteract the tumor immune response, further promoting the development of resistance.
Although targeted therapy and immunotherapy have achieved some clinical success, the development of resistance remains a significant challenge. Due to the inevitable resistance, even these latest cancer treatment methods cannot be used repeatedly to treat cancer, and in the long term, they seem fleeting and unable to defeat cancer.
On the other hand, as can be seen from the table below, regions with much better cancer treatment conditions than China do not show a significantly lower cancer mortality rate compared to China, suggesting that modern cancer treatment methods have a limited effect during the fight against cancer .
Five Key Factors in Cancer Treatment: The Emergence of Chlorine Dioxide Intratumoral Injection
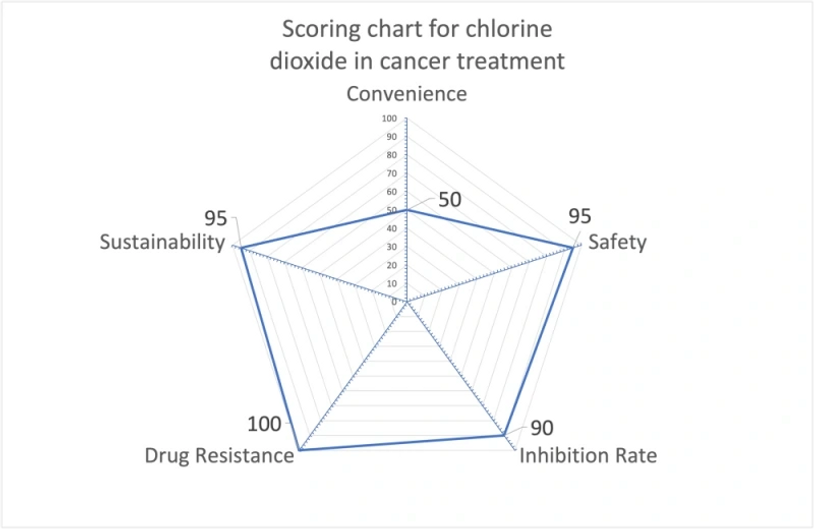
To evaluate the effectiveness of a cancer treatment method, it is crucial to consider five key factors: convenience, safety, inhibition rate, drug resistance, and treatment sustainability. For instance, while oral chemotherapy drugs offer convenience, they have drawbacks in terms of safety, inhibition, and drug resistance. On the other hand, surgical treatment demonstrates excellent results in inhibition and drug resistance, but its convenience and sustainability are limited due to infrequent repetition. Radiation therapy provides moderate inhibition, drug resistance, and good sustainability, but it scores low in convenience and safety. As a result, it is suitable for treating cancer at different stages. Targeted drugs and immune checkpoint inhibitors face challenges related to drug resistance and sustainability. Although they can extend patients’ survival for a period, unfortunately, many patients still succumb to the disease.
An ideal cancer treatment should excel in all five aspects, potentially transforming cancer into a chronic disease or even achieving a complete cure. However, current major cancer treatment methods do not score highly in all these dimensions. To improve scores in each aspect, modern medical technology often focuses on specific dimensions. For example, directly injecting chemotherapy or immunotherapy drugs into the tumor can significantly enhance safety and inhibition rates at the expense of convenience.
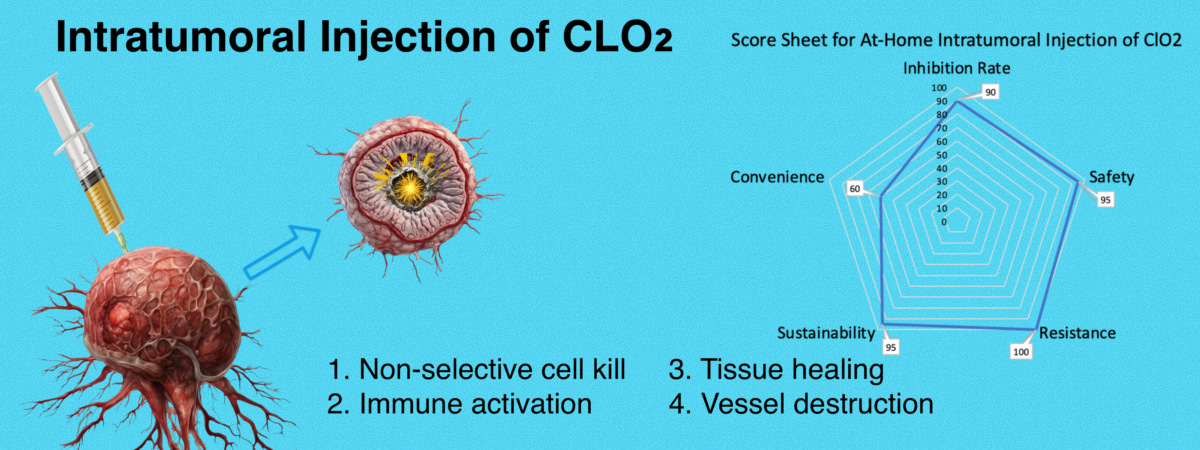
Therefore, when evaluating an ideal cancer treatment approach, it is essential to consider the five key dimensions: convenience, safety, inhibition rate, drug resistance, and treatment sustainability. Taking into account our preclinical research results, it is evident that intratumoral injection of chlorine dioxide for cancer treatment excels in all five aspects, making it an optimal approach for cancer treatment.
Chlorine Dioxide as a Targeted Cancer Therapy: Harnessing ROS-like Properties for Improved Outcomes
Our team is currently investigating the use of chlorine dioxide for cancer treatment. Chlorine dioxide shares similar properties with powerful oxidizing agents known as ROS, which have been shown to destroy cancer cells and aid in tissue repair. We have discovered that chlorine dioxide can be safely used as a therapeutic agent in humans. Our research focuses on delivering chlorine dioxide directly into tumors as an innovative approach to cancer treatment. By targeting the tumor directly, chlorine dioxide can specifically kill cancer cells without promoting drug resistance. Additionally, chlorine dioxide has demonstrated the ability to stimulate an immune response against cancer, further enhancing its therapeutic effects. Our goal is to extend the lives of patients and transform cancer into a manageable chronic illness by injecting chlorine dioxide directly into tumors. This groundbreaking treatment utilizes the ROS-mimicking abilities of chlorine dioxide to eliminate cancer cells and promote tissue regeneration. By harnessing the unique properties of chlorine dioxide, we offer a new pathway to improve patient outcomes in cancer treatment. Ongoing studies are necessary to refine the delivery methods and dosage of chlorine dioxide, as well as explore its combined effects with other treatments. As research progresses, direct tumor injection of chlorine dioxide emerges as an exciting and promising approach to effective cancer therapy.
The Preclinical Research
To learn more about this preclinical research.

TO LEARN MORE ABOUT THIS PRECLINICAL RESEARCH
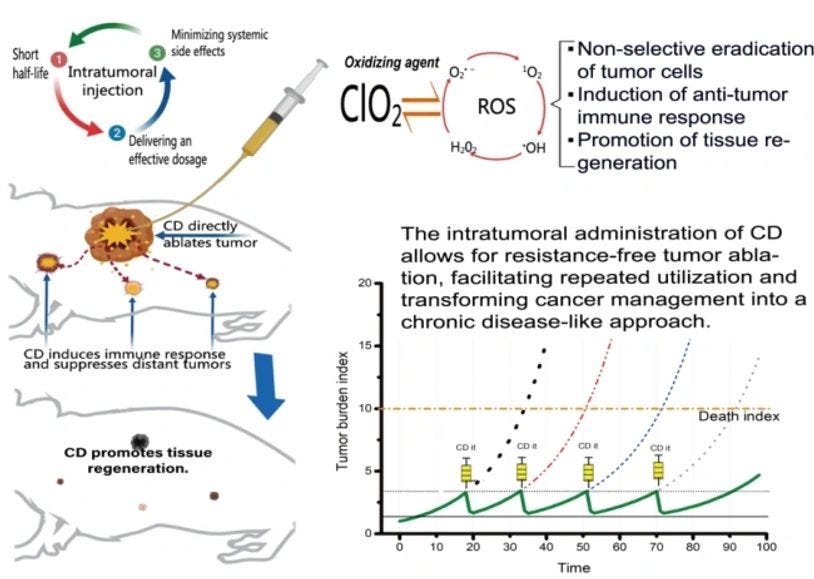
The Primary Mechanisms of Intra-Tumoral Chlorine Dioxide (CD) Therapy for Treating Cancer
Direct Destruction of Cancer Cells:
CD’s strong oxidative properties allow it to kill cancer cells upon, a significant advantage over other injectable drugs (including intratumoral drugs and oncolytic viruses). With intra-tumoral therapy, we don't need to worry about maintaining CD in the tumor long periods, which a big challenge for many existing treatments.
Destruction of Tumor Blood Vessels:
High concentrations CD can directly damage tumor blood vessels. This means the tumor tissue doesn’t need to be completely saturated with CD; untreated tumor cells will die to lack of energy.
Induction of Systemic Anti-Tumor Immune Response:
CD can trigger a systemic immune response against tumors. In theory, patients don’t need to inject every single tumor. For small, untreated tumors at distant sites, CD’s systemic anti-tumor immune can effectively inhibit these small tumors.
Promotion of Tissue Regeneration:
CD has a mechanism that aids in tissue regeneration. For patients with advanced cancer, this is crucial because the reason they can't undergo surgery is the inability to heal large wounds post-tumor removal. When patients use CD, it can help regenerate tissue and heal any wounds formed tumor ablation.
We envision a method of using CD for periodic and intermittent tumor ablation. This approach starts intra-tumoral injection ablation treatment when the tumor burden reaches a clinically observable level. After CD ablates the tumor, it not only has a direct ablation effect but also does not cause drug resistance and can enhance immune capacity. This keeps the tumor burden within a safe range, transforming cancer with solid tumors into a true chronic condition where patients do not die from cancer.
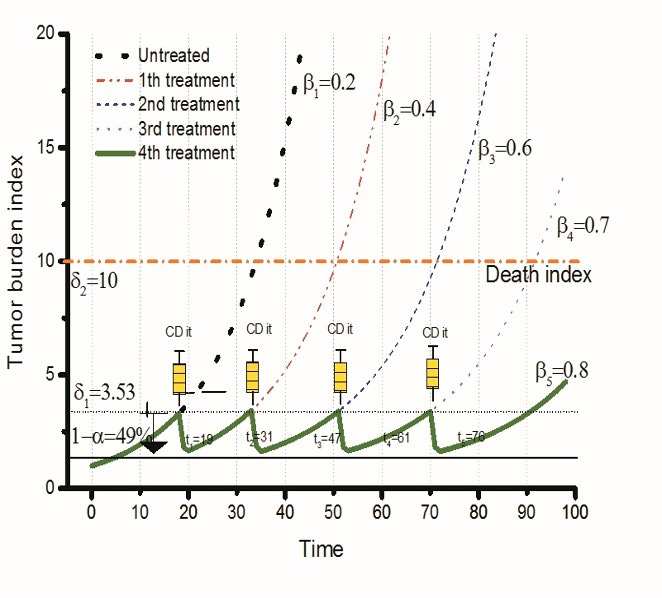
Each ablation reduces the tumor burden (α=51%) and enhances immune capability, ensuring that the tumor burden curve never reaches the mortality line
Why Late-Stage Breast Cancer Patients Should Consider Intratumoral Chlorine Dioxide Injections First
While intratumoral injections can be challenging, especially without a doctor's support, it is entirely feasible for some patients to self-treat at home for superficial cancers. For example, breast cancer patients can easily perform injections into primary or lymph node metastases with the assistance of a family member.
I recommend that late-stage breast cancer patients try intratumoral chlorine dioxide injections for self-treatment to circumvent the limitations of modern medicine, which can adequately treat early-stage breast cancer but struggles with advanced cases.
Currently, there are approximately 2.2 million new breast cancer cases annually worldwide, with around 680,000 deaths. Considering a 5-year survival rate of 25% for stage 4 breast cancer, it is estimated that around 2.3 million patients are in the late stages each year. I believe these patients have been largely abandoned by modern medicine.
.
https://andreaskalcker.com/en/publications-in-humans/